
Does your healthcare organization have an enterprise-level strategy for all your patient communications?
This is a good question because a basic communication process has three key layers to it:
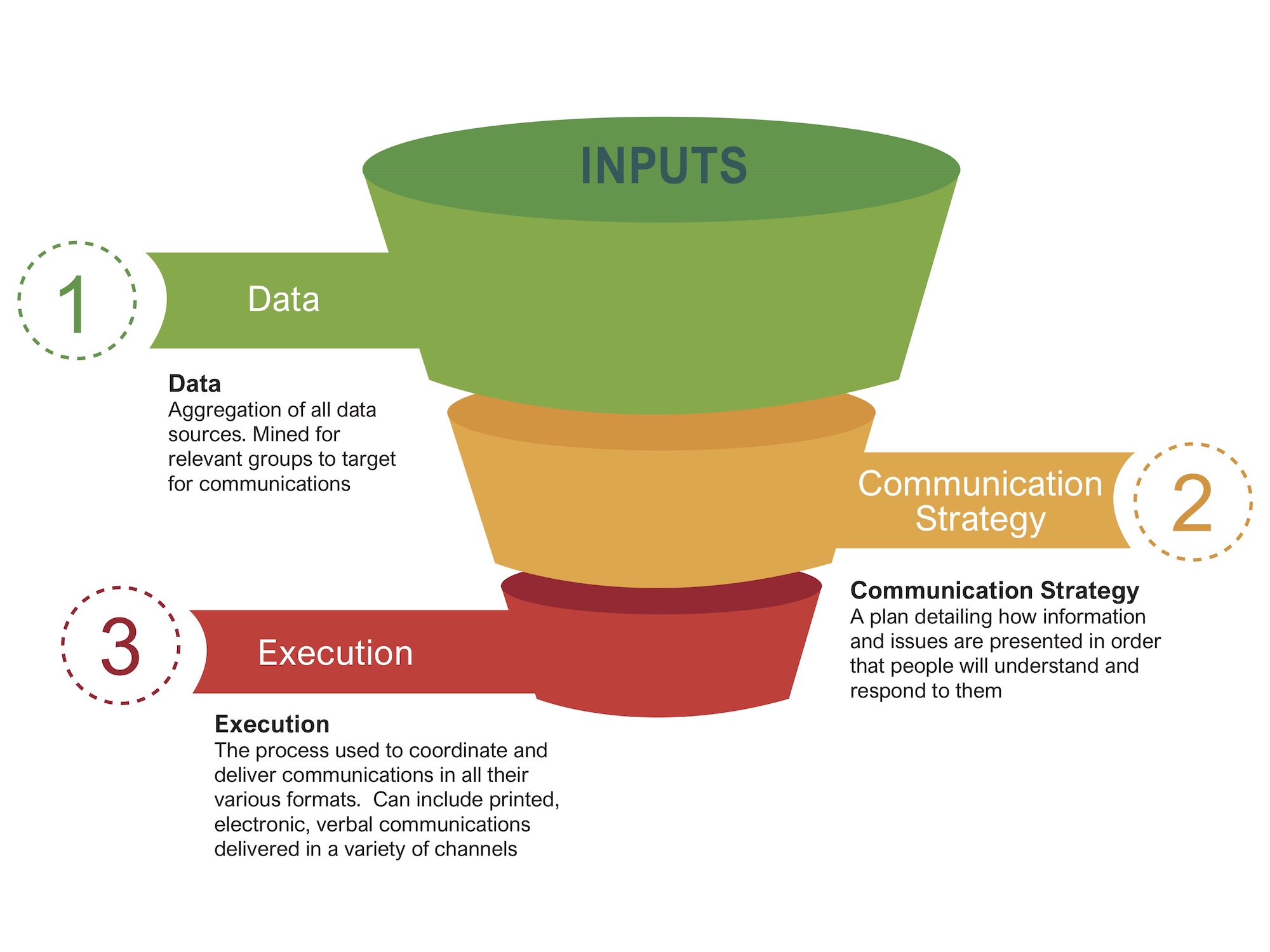
- Raw data that forms the knowledge about your patients.
- A communication strategy designed to take that knowledge and transform it into a message.
- Execution activities to create and deliver the desired communications in a variety of formats.
Multiple organizations interact with a patient during their healthcare journey. This complicates the communication process. It is even more complex for the chronically ill who frequently interact with a wider variety of medical personnel. With clean data, well-defined strategy and effective execution, you are destined to a future of successful patient communications. Otherwise, you risk fragmented and disorganized communications, care, and health outcomes.
Three points of potential success
I’ll start by simplifying this discussion and break out the three layers: data, communication strategy, and execution. Take a look at the following graphic:
What do you actually know?
Data is the starting point for any discussion on how you communicate with your patients. But a great deal of it is focused on clinical activities and housed in an EHR system. Even if you have nonclinical data, is it incorporated in the patient record or is it part of a third-party application or platform? Is it set up in a way that allows you to access and use it easily? I mentioned in an earlier post a great deal of data is used for push communications to patients. A two-way communication process pushes data and communications out to patients and elicits patient feedback on the accuracy of your data. This is important because patient preferences change, health literacy improves, or patient conditions change. What works today may not work tomorrow, which impacts the accuracy of patient data and preferences. A process that does not continually test the accuracy of data you have on patient preferences and interests is essentially a recipe for sub-optimal health care and outcomes.
Who owns the strategy?
The second layer to this graphic is communication strategy. It is an enterprise level strategy for how you will use patient data to interact with your patient population. It is not a departmental strategy. This is a really important distinction because many organizations have their communication touchpoint strategies managed by a variety of business owners in different departments. Each business owner might decide to communicate to patients via web based platforms, phone apps, email, other electronic channels or paper mail. There is also strategy fragmentation on the clinical side. Primary care physicians may not be in the same organization as the specialists or therapists. Each may belong to an organization that has its own communication strategy. Without an overall plan, patients may experience different business owners and businesses delivering competing and conflicting messages via channels that don’t resonate with your target population. Who owns the overall patient communication strategy? In many cases, no one.
Time for Action
The third layer to this graphic is the most critical. You may have accurate and comprehensive health and personal patient data. You may have a good communication strategy in place for chronically ill populations. Now you have to execute it. Execution means accessing the data and efficiently using it to deliver information to patients in the right format and at the right time. You then capture patient feedback in a two-way communication process. Even more, many applications and platforms used to execute communications are from different vendors. The apps platforms don’t interact with each other, nor do they have a common interface to execute the strategies. Health system consolidation is adding to these issues because now you could have duplicate applications that do not work with each other, all trying to do the same thing. Execution is hairy. How do you manage that?
All for one or one for nothing
Each of the three layers of a communication process must work efficiently or the process breaks down. If you have outdated data, it doesn’t matter how good your communication strategy and execution are. The communications will not resonate. When you have highly accurate data with up-to-date information on patient preferences, it won’t matter if you have a poorly thought out or fragmented communication strategy, or if your execution process is broken. Health care organizations are investing a great deal of money and time tying together clinical activities as part of coordinated care or accountable care organizations. The same process needs to occur for communication because it is currently just as fragmented.
As I mentioned in previous posts, communication breakdown really doesn’t affect the majority of health care encounters because most are related to symptoms resolved in one visit to the doctor. The breakage most dramatically affects chronically ill populations who generate the greatest amount of expense for our health care system. Every effort should be put forth to figure out (1) how to tie all three communication layers together efficiently and (2) align them with initiatives to coordinate care across chronically ill populations. Accountable care without accountable communications will never work as effectively as it is intended to for chronically ill populations. This is especially true when it comes to the newer focus on population health. If we can use data to slice and dice patients into meaningful groups and target them with population-based treatment, then we can do the very same with communications. I’ll talk about this in subsequent posts.
Do you have coordinated communications?
I’ll leave you with the following thoughts. If you are truly committed to an enterprise-level approach for patient communication, you need to start today by asking yourself the following questions regarding your current and future state.
Data:
- Where is our patient data stored across the enterprise?
- Is it accessible and secure in all clinical and non-clinical forms?
- Do we have a process that checks the accuracy of that data and adds to the depth of knowledge we have for each patient?
Communication Strategy:
- Who owns the communication strategy for every patient touchpoint that is created in our organization?
- How is messaging coordinated across chronically ill populations?
- Does the strategy address patient barriers with respect to language, education and culture that prevent them from achieving a level of health literacy necessary to manage their own health?
Execution:
- How are we executing each and every one of these communications?
- What mix of internal applications versus external vendors are we utilizing to deliver these communications?
- How many duplicate applications are running due to consolidation with other health systems?
- What is our long term strategy for generating consistency of execution through a standardized set of applications or vendors?
The entire healthcare ecosystem both in clinical and non-clinical environments is driven by data, strategy, and execution. We need the same focus for communications to ensure that chronically ill populations have the health literacy necessary to improve outcomes and lower cost.
No Comments